http://www.eurekalert.org/pub_releases/2014-05/uocd-rwc053014.php
A study presented at the American Society of Clinical Oncology (ASCO) Annual Meeting 2014 reports the results of a first-in-human, phase 1 dose escalation trial of crizotinib (XALKORI) in 14 patients with advanced, MET-amplified non-small cell lung cancer (NCT00585195).
In 2011, the drug crizotinib earned accelerated approval by the US FDA to target the subset of advanced non-small cell lung cancers caused by rearrangements of the anaplastic lymphoma kinase (ALK) gene, and subsequently was granted regular approval in 2013. The drug also has shown dramatic responses in patients whose lung cancers harbored a different molecular abnormality, namely ROS1 gene rearrangements. Previously unreported phase 1 clinical trial results now show that crizotinib may have a third important molecular target. In advanced non-small cell lung cancer patients with intermediate and high amplifications of the MET gene, crizotinib produced either disease stabilization or tumor response. Sixty-seven percent of patients with high MET amplification showed prolonged response to the drug, which lasted from approximately 6 months to nearly 2.5 years.
"Though more patients are needed to really pin down the exact MET criteria that will predict benefit from MET inhibition, we're hopeful this line of research will define yet another key molecular subtype of lung cancer sensitive to a targeted drug," says Ross Camidge, MD, PhD, director of the thoracic oncology clinical program at the University of Colorado Cancer Center and the study's lead author.
Crizotinib showed early activity against MET-dependent cells in preclinical laboratory studies, and the phase I clinical trial design included plans for treatment of cancer patients preselected for evidence of MET activation once the recommended dose was determined.
Matching the drug to MET amplifications required testing for this genetic abnormality in patient tumors, something that hasn't been part of standard lung cancer screening in most clinical centers. Working at the CU Cancer Center, Marileila Garcia, PhD, was able to rapidly deploy an assay for MET for the trial based on fluorescent in situ hybridization (FISH).
Garcia's previous work, also shown for the first time in this presentation, gives insight into the frequency of MET amplification in lung cancer. Consistent with other reports, Garcia found some degree of MET amplification present in 7.4 percent of 800 consecutive samples of non-small cell lung cancer tested at the Colorado Molecular Correlates Lab from 2009 to 2012. However, the level of MET amplification in these samples was not uniform. Low MET amplification (MET/CEP7 ratio of ≥1.8-≤2.2) was present in 3.8 percent, intermediate amplification (MET/CEP7 ratio of >2.2-<5.0) was present in 3 percent, and high amplification (MET/CEP7 ratio of >2.2-<5.0) was present in 0.8 percent.
In the phase 1 clinical trial, while disease in the 2 patients with low MET amplification did not appear to benefit from the drug, 1 of 6 patients with intermediate MET amplification achieved a partial response with 4 of the 6 having more minor responses (stable disease), and in the high MET amplified group 1 of 6 achieved a complete response, 3 of 6 achieved a partial response and 1 of the 6 had a minor response (stable disease). Overall objective response rates in the low, intermediate and high MET amplified cohorts were 0, 17 and 67%, respectively.
"We've been through a similar experience with ALK-positive lung cancers - patients whose cancers depend on a specific molecular abnormality can see significant benefit when we remove the cancer's access to the driving abnormality," Camidge says. "However, unlike classical activating mutations or gene rearrangements, MET is likely to be a more challenging biomarker because it is not simply black or white - not simply off or on - but rather it is a continuous variable. Although the dataset is still pretty small, there is a strong suggestion that a definable cut-point in MET amplification exists which could really delineate who will or will not benefit from this drug. Screening for MET amplification and treating these patients in clinical trials is the only way we will be able to discover this important threshold."
The implications of crizotinib used to target MET amplifications may go beyond non-small cell lung cancer. The gene is activated in many different ways in many different cancers, and patients with MET-amplified cancers continue to enroll in the crizotinib phase I study.
"With these targeted therapies, it can look at first like a drug may only be useful to a small percentage of patients with the targeted genetic abnormality. But then you start to see the same abnormality across cancer types and the drug that looked like it might have been useful in, say, 3 percent of lung cancer patients, turns out to have a use in x-percent of all these other cancer types as well. It's a new paradigm: we're working to pick off these molecular aberrations one by one," Camidge says. |
 奥西替尼耐药后续治疗,出现腹水
治疗经过:
2010确诊腺癌
治疗方案:右肺上叶切除,10年民诺宾2次,顺铂+盖诺2次。
奥西替尼耐药后续治疗,出现腹水
治疗经过:
2010确诊腺癌
治疗方案:右肺上叶切除,10年民诺宾2次,顺铂+盖诺2次。
 三代伏美换一代特罗凯获益率问题
家父25年2月因肩膀疼痛确诊肺腺癌晚期4B,双肺转,多发骨转,脑转(非典型),
三代伏美换一代特罗凯获益率问题
家父25年2月因肩膀疼痛确诊肺腺癌晚期4B,双肺转,多发骨转,脑转(非典型),
 盲试靶向药 29个月,治疗分享
时间:2025/1/27 盲试靶向药第29个月。
本月治疗方案:7080(14mg)。2024年11月底
盲试靶向药 29个月,治疗分享
时间:2025/1/27 盲试靶向药第29个月。
本月治疗方案:7080(14mg)。2024年11月底
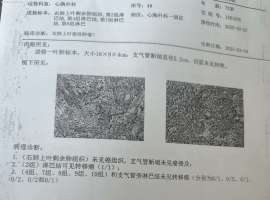 完成手术,病理也出来了,烦请各位老
之前因为心脏问题,去心内造影,前降支75%狭窄,回到心胸外科手术,目前主治医生说是
完成手术,病理也出来了,烦请各位老
之前因为心脏问题,去心内造影,前降支75%狭窄,回到心胸外科手术,目前主治医生说是
 生存期超4年!首个击败奥希替尼的药
作者:seacat
2025年3月26日,巴黎举行的2025欧洲肺癌大会(ELCC 2025)报道了III期研
生存期超4年!首个击败奥希替尼的药
作者:seacat
2025年3月26日,巴黎举行的2025欧洲肺癌大会(ELCC 2025)报道了III期研





 显身卡
显身卡


